
Tunnel syndromes are comparable in symptoms yet are very distinguishable in their characteristics. Many symptoms overlap with numbness and pain, but the locations are the key determinates. While all three of the nerves start in the neck, they travel down the arm and take different paths. Where the pain starts in the arm can determine which nerve is the problem.
The two main nerves are the median nerve in the wrist and the ulnar nerve in the elbow. One nerve could be affected, causing partial hand numbness, or both nerves could be affected, causing numbness in the whole hand. The numbness can be intermittent or constant. A third nerve issue, which is less common, is the radial nerve, radiating pain to the back of the hand, thumb, middle, and index fingers (see images 1, 2).
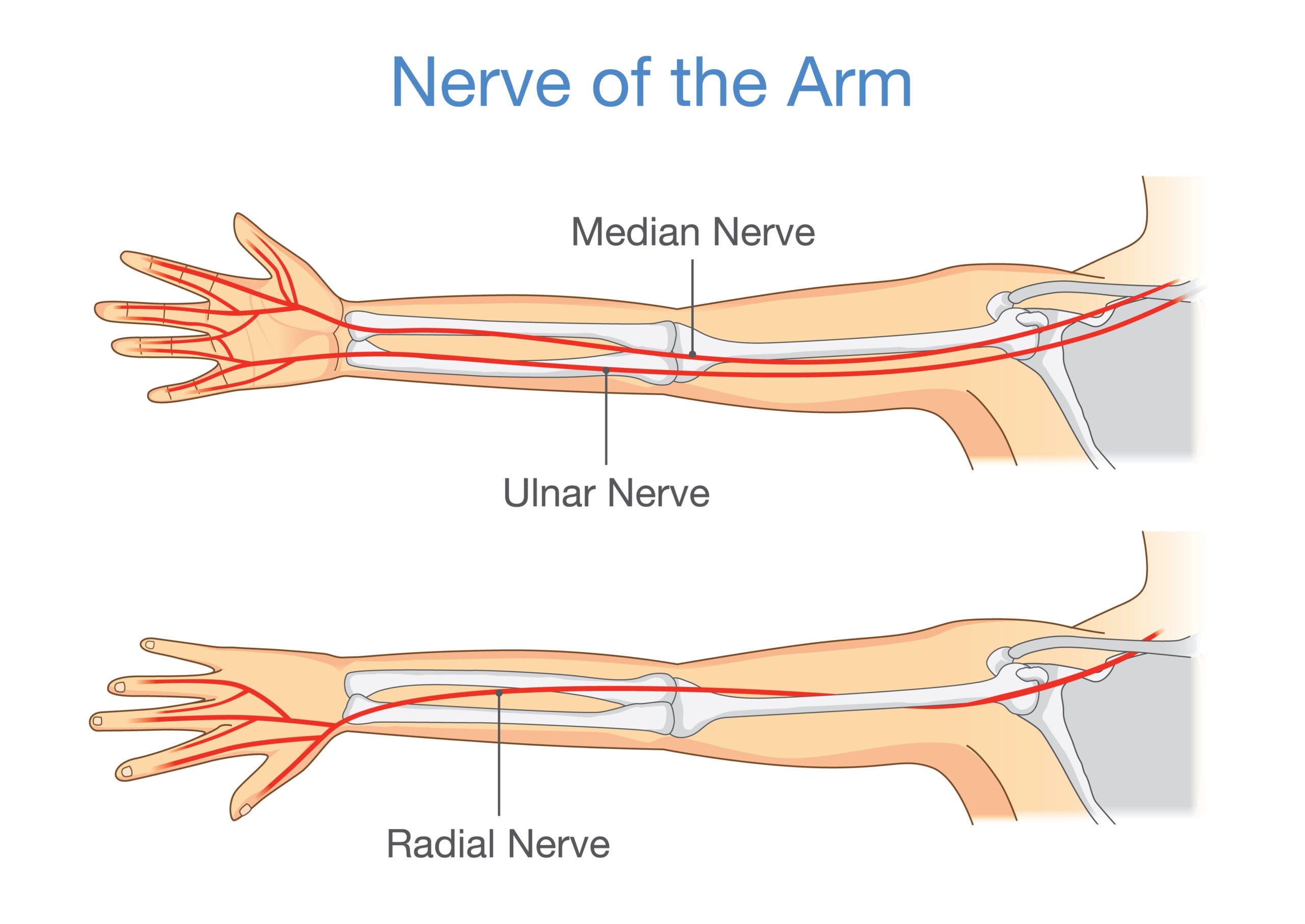
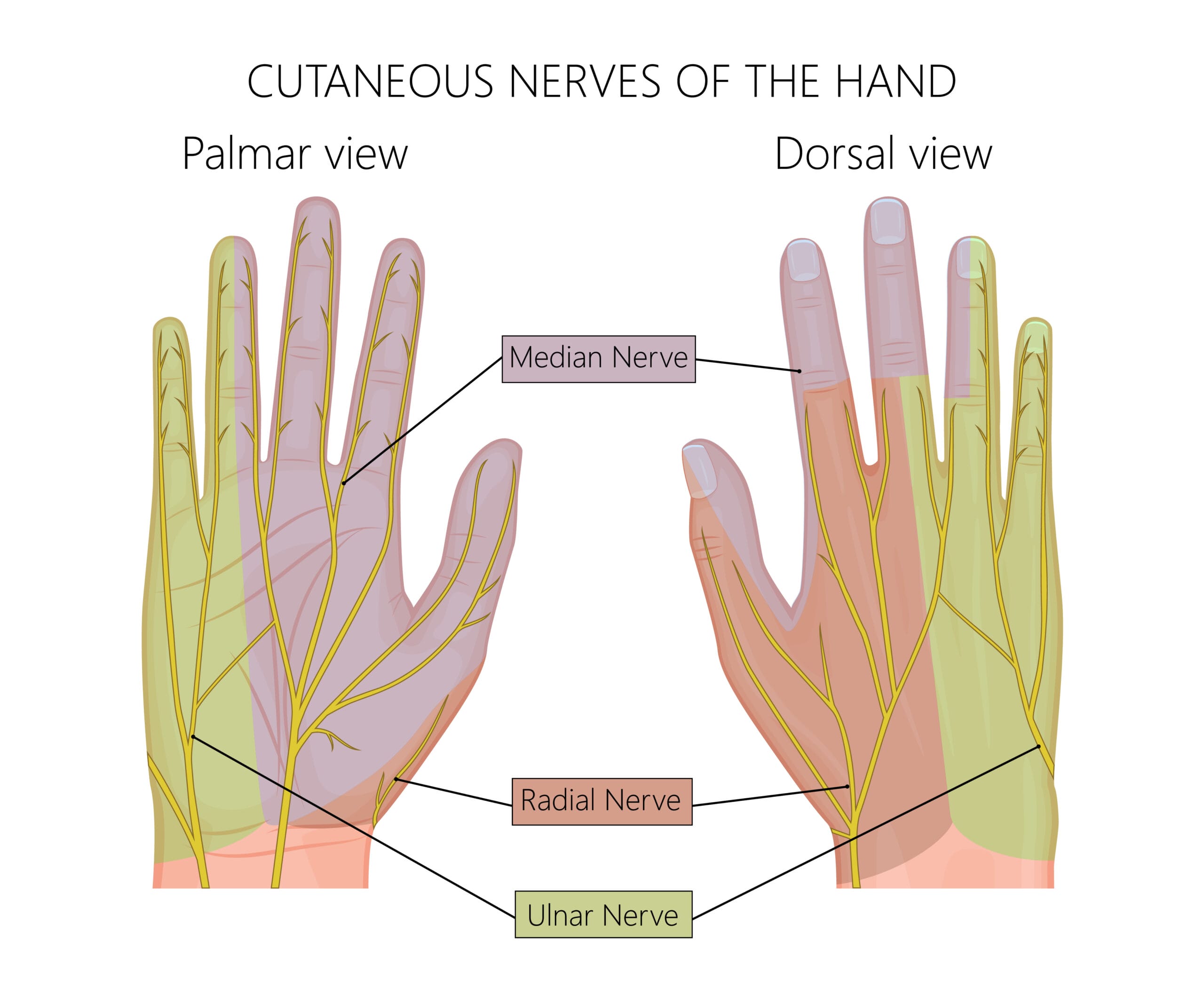
Image 2: Nerves of the hand | © Aksana / Adobe Stock
Median Carpal Tunnel Syndrome
The median nerve is the focus of the most common carpal tunnel syndromes. Originating in the neck from a group of nerve roots, it then runs together to form one nerve to pass down the arm and forearm to the wrist. The median nerve travels through the carpal tunnel through the wrist to the thumb, index, middle and half the ring finger. This nerve controls sensation and movement in the hand. When the median nerve is pinched, entrapped, or inflamed, it causes numbness.1
The first symptoms of carpal tunnel syndrome are numbness during the nighttime as the wrists are usually bent during sleep. It comes on gradually without any specific injury.
Symptoms originally appear sporadic, and, as it worsens, the symptoms will occur often and lingers. As the condition progresses, numbness is experienced with more simple daily activities like driving, styling hair, applying makeup, using the phone, sewing, reading a book, computer work, or in the case of dental hygienists, during scaling. It appears more so in the dominant hand but will also be in both hands.

The biological cause of carpal tunnel syndrome starts with the swelling of the tenosynovium ─ a protective lining of tendons. When these tendons swell by the pressure of the carpal tunnel narrowing, it causes a buildup of synovial fluid. This is the natural lubricant the body makes to protect the tendons within the carpal tunnel. In response to the fluid buildup in the wrist, the transverse ligament becomes thicker and wider to cause pressure onto the median nerve, altering adequate blood supply and oxygen for proper function. This is when symptoms will be noticed.
Several factors can cause carpal tunnel syndrome:
- Anatomy of the wrist ─ the shape of the bones, or arthritis to compress the nerves
- Trauma ─ fractures, dislocations, tumors, or cysts change the structure of the wrist’s bones and muscles
- Pregnancy ─ hormonal changes, edema, and fluid retention can increase chances of carpal tunnel syndrome and subside after birth
- Menopause ─ hormonal changes cause fluid buildup and more likely if there was an occurrence during pregnancy
- Gender ─ women have smaller wrists
- Health conditions ─ hypothyroidism, obesity, rheumatoid and osteoarthritis, gout, musculoskeletal disorders, chronic kidney insufficiency
- Diabetes ─ uncontrolled high blood sugar correlates with neuropathy, and glucose is believed to attach to tendons to enlarge them and cause compression within the carpal tunnel
- Medications ─ affect the immune system and blood thinners
- Tobacco ─ lowers the immune response and increases inflammatory diseases and fluid buildup
- Hereditary ─ smaller boned people are more likely to have wrist and bone structures where median nerve compression is more vulnerable. If a sibling or parent develops it, it increases the chances of other family members.
- Age ─ aging musculoskeletal disorders are more prominent
- Occupation ─ knitters, carpenters, bakers, mechanic, dental, painter, and many more
- Mechanical stress ─ involving repetition, vibration, strong gripping, heavy lifting. repetitive and awkward hand motions.2,3
Symptoms include numbness, tingling, burning pain in the wrist, shock-like sensations radiating into the fingers, weakness, and clumsiness (challenging to perform fine motor functions such as buttoning clothes and nonsurgical periodontal treatment), dropping things, and hot and cold sensations.3
Diagnosis
Early diagnosis is important as carpal tunnel worsens over time. If left untreated, it may cause permanent damage to the nerves, contributing to numbness and muscle atrophy in the hands. The physical examination to test for carpal tunnel syndrome checks for tingling and numbness, as well as:
- Tinel sign (tapping along the median nerve for finger sensation)
- Bending and holding the wrist in a flexed position to check for hand sensation
- Testing sensitivity by lightly touching the fingers with the patients’ eyes closed
- Checking muscles around the base of the thumb for weakness and atrophy
Other tests may also be involved beyond the physical examination, including:
Electrophysiological tests the pressure and how well the median nerve functions. This includes the nerve conduction test to determine the nerves of the hand and arm and how efficiently they respond to a minor electrical zap. Along with this, an electromyogram is conducted to measure the electrical activity in the muscles to determine nerve and muscle damage.
Ultrasounds are high-frequency sound waves of the bone and tissue and can evaluate for signs of compression on the median nerve.
X-rays provide images of dense structures such as bone to eliminate the possible cause of arthritis, fractures, or ligament injury.
MRIs provide images of soft body tissue to eliminate other causes of abnormal tissues that may be compressing the median nerve, such as scarring, injury, or tumors.
Treatment
As with many conditions, the conservative approach is initially recommended. Mild carpal tunnel can be treated by wearing a wrist splint during the night. The splint holds the wrist in a straight position to keep room in the carpal tunnel for the nerve to rest.
Wrist and hand exercises, as well as stretches and nerve gliding exercises, help the nerve move better, and nonsteroidal anti-inflammatory medicines for early symptoms aid in reducing swelling and pain.
Other treatment options are:
- Bracing or splinting for the wrists to keep them straight
- Steroid injections for an anti-inflammatory to relieve symptoms and flare-ups
- Change in activities to slow or stop the progression
Surgery is the most definitive treatment in median carpal tunnel. The ideal is to release the pressure of the median nerve in the carpal tunnel. The two surgeries that do this cut the transverse carpal ligament to open the size of the carpal tunnel to decrease pressure on the median nerve. Open carpal tunnel release is when small incisions are made on the palm to open the wrist and divide the transverse carpal ligament. Endoscopic carpal tunnel release is when two smaller skin incisions are made, and a small camera and knife are used to cut and divide the transverse carpal ligament.3
A similarity in symptoms appearing with other conditions can lead to misdiagnosis.
Arthritis can affect all fingers and hands ─ felt throughout the day. The pain is constant and may be triggered and intensified if a strain is applied to the wrist and hands. Carpal tunnel syndrome does not affect the pinky finger and worsens at night; the symptoms can be absent then come on suddenly by certain activities.
Nerve compression related to the spine as a slipped disc and cervical stenosis causes weakness and numbness. The condition affects the neck, shoulders, hands, arms, and legs, and nerve compression mimics similar sensations of carpal tunnel syndrome.
Wrist tendonitis includes pain, tingling, and numbness, affecting the tendons in any part of the hand and wrists. With carpal tunnel syndrome, the pain, tingling, and numbness are specific to the thumb, index, and middle finger, the palm side of the wrist, and half the ring finger.
Thoracic outlet syndrome is compressed blood vessels or nerves located in the collarbone and the first rib. The shoulders, neck, and fingers are affected. As mentioned above, carpal tunnel syndrome affects the thumb, index, and middle finger, the palm side of the wrist, and half the ring finger.
Repetitive strain injury is a general term and can affect any part of the body. But it is mostly concentrated in the neck, shoulders, forearms, elbows, hands, and wrists. Muscles and tendons feel pain, throbbing, and stiffness from overuse and repetitive movements. It can be misdiagnosed for carpal tunnel syndrome when it is in the hands and wrists.3
Cubital Tunnel Syndrome
The ulnar nerve is the main character in the cubital tunnel. This nerve runs through the cubital tunnel at the elbow and travels to half of the ring finger and the whole pinkie finger. This is more challenging to diagnose as the elbow seldom presents pain.
Mild cases of cubital tunnel syndrome can be treated with protective strategies. When the elbow is straight, it provides the most room for the ulnar nerve. When bent, it pulls the nerve taut and stresses the nerve.
Causes for cubital tunnel syndrome include:
- Repetitive or prolonged activities with the elbow bent
- Prior injury or fracture of the elbow
- Swelling, cyst, arthritis of the elbow
- Bone spurs at the elbow
Cubital tunnel syndrome symptoms occur with the ringer and pinkie fingers and can include:
- Weakness
- Tingling
- Numbing
- Unable to grip
- Increase in dropping things such as instruments
There are a few ways to test for cubital tunnel syndrome.
Imaging tests such as x-rays are used to determine dense bone structure to rule out bone spurs, arthritis, or other bone issues that could be causing compression of the ulnar nerve.
Nerve conduction tests determine the response of the nerve and basically how alive the nerve is. The quicker it responds to electrical pulses, the healthier the nerve. Whereas a slower response means the nerve isn’t functioning well. This testing also determines muscle damage which is a sign of severe nerve compression.4
Treatment recommendations typically include:
- Nonsteroidal anti-inflammatory medicines for early symptoms to aid in reducing swelling
- Steroid injections may be recommended but are not commonly used as they may increase the risk of damage to the nerve
- Bracing or splinting whenever possible, usually at night, to keep the elbow straight
- Nerve gliding exercises to help the ulnar nerve slide through the cubital tunnel and the Guyon’s canal in the wrist to improve symptoms and stiffness in the arm and wrist
- Avoid activities that require bending of the elbows for a long time. Keeping the elbow straight as often as possible allows the openness for the nerve to function
- Restrain from leaning on the elbow, which can put undue stress and pressure on the elbow and ulnar nerve
The reasons for surgery would be if nonsurgical treatments have not improved the condition, the ulnar nerve is severely compressed, and muscle weakness or damage has occurred. Surgery is the definitive treatment to relieve nerve entrapment at the elbow and is recommended more so for moderate to severe cases of nerve compression to prevent nerve damage. Failure or waiting too long to have surgery can result in permanent nerve damage, numbness, muscle loss, weakness, and loss of function. Surgery has a high success rate, and on average, 87% of people see good improvements.
A type of surgery is cubital tunnel release when the ligament in the cubital tunnel is cut and divided. This technique expands the size of the tunnel and decreases the pressure on the nerve. The healing process of the ligament starts with new tissue growth to allow more space for the ulnar nerve to slide. This surgery works best for mild or moderate nerve compression.
Ulnar nerve anterior transposition is the other type of surgery and is used when the ulnar nerve has displaced itself from behind the medial epicondyle to the front of it. Transferring the nerve to the front of the medial epicondyle prevents it from catching on the bony ridge; this happens when the elbow is stretched or bent.5
The clinician should differentiate from other conditions that cause the same symptoms, leading to a misdiagnosis. Golfer’s elbow, known as medial epicondylitis, has tenderness to palpitation directly over the medial condyle. On the other hand, cubital tunnel syndrome has tenderness to palpitation over the ulnar nerve about one inch below the medial epicondyle.6

Radial Tunnel Syndrome
Radial tunnel syndrome is compression of the radial nerve. This nerve is on the opposite side of the ulnar nerve. It starts in the neck area at the brachial plexus travels through the triceps to the outside of the elbow. It is one of three nerves along the bones and muscles of the forearm and elbow, providing motor and sensory functions.
The radial nerve is responsible for the extension of the arm, wrist, and fingers and the outward rotation of the forearm. It provides movement to the muscles of the back of the forearm and the sensation of the skin of the forearm and the back of the hand. This type of tunnel syndrome is less common than cubital and carpal.7
Some causes for radial tunnel syndrome include:
- Injury to the forearm, constant wrist-twisting motions
- Poor arm strength and flexibility, lack of warming up before exercising
- Diabetes
- Underactive thyroid gland
- Noncancerous fatty tumors or ganglion cysts
- Inflammation, swelling, or fluid retention of the surrounding tissue
- Bone tumors and fractures
Radial tunnel syndrome symptoms can include:
- Pain, cutting, piercing, stabbing at the top of the forearm or back of the hand, more so when the wrist and fingers are straightened.
- Pain will increase with activity related to heavy lifting or extending the elbow and rotating the forearm inward
- Tenderness in the upper forearm
- Pain is present a few inches below the outer part of the elbow
Unlike the cubital and carpal tunnel syndromes, numbness or tingling is rare as the radial nerve affects the muscles.
The pain in the forearm and hand are the main symptoms. It’s commonly diagnosed by a physical examination of resistance with the hands, middle finger, and arms to locate the pain. If there is pain with resistance, it’s a sign of radial tunnel syndrome. Other tests may be done as x-rays on the elbow, MRI of the spine, and electromyography and nerve conduction.
Treatment options typically follow this pattern:
- In mild cases, physical therapy, avoiding pressure on the elbow, wearing a splint or elbow pad
- Nonsteroidal anti-inflammatory medicines for early symptoms to aid in reducing tissue swelling
- Corticosteroid injections to relieve inflammation and pressure on the radial nerve
- Exercises, nerve gliding, stretches, and strengthening
- Alternating hot/cold
- Ultrasound
- Ergonomic improvements
If these initial therapies are not effective, then radial tunnel release surgery is needed. Compressive sites will be divided within the radial tunnel. This increases space in the tunnel promoting new tissue growth across the split and developing a permanently larger tunnel.7
Differentiate from other conditions that cause the same symptoms and lead to a misdiagnosis. An example is tennis elbow (lateral epicondylitis), which is the inflammation of tendons of the outside of the elbow as pain radiates to the forearm and wrist. Pain is felt when the wrist is bent. Radial tunnel syndrome affects the radial nerve with pain. To determine whether it is the radial nerve, pain is centered about two inches down the arm, where the radial nerve goes into the supinator muscle.
Preventing and managing tunnel syndrome as a dental professional is important for longevity in the job. Gripping relatively thin instruments with force on a day-to-day basis creates repetitive stress in the fingers, hands, wrists, and forearms may eventually cause a tunnel syndrome. Being aware of symptoms early on to prevent or treat can prolong a satisfying dental career.
Before you leave, check out the Today’s RDH self-study CE courses. All courses are peer-reviewed and non-sponsored to focus solely on high-quality education. Click here now.
Listen to the Today’s RDH Dental Hygiene Podcast Below:
References
- Faust, K., Jennings, C.D. (2016, July). Carpal tunnel Syndrome. OrthoInfo: American Academy of Orthopaedic Surgeons. Retrieved from https://orthoinfo.aaos.org/en/diseases–conditions/carpal-tunnel-syndrome/
- Carpal Tunnel Syndrome. (2021, September 22). Canadian Centre for Occupational Health and Safety. Retrieved from https://www.ccohs.ca/oshanswers/diseases/carpal.html
- Carpal Tunnel Syndrome (CTS). (2019, December 19). Retrieved from https://ada.com/conditions/carpal-tunnel-syndrome/
- Athwal, G.S., Keener, J.D. (2020, August). Ulnar Nerve Entrapment at the Elbow (Cubital Tunnel Syndrome). Ortho Info. Retrieved from https://orthoinfo.aaos.org/en/diseases–conditions/ulnar-nerve-entrapment-at-the-elbow-cubital-tunnel-syndrome/
- Wade, R.G., Griffiths, T.T., Flather, R., et al. Safety and Outcomes of Different Surgical Techniques for Cubital Tunnel Decompression: A Systematic Review and Network Meta-analysis. JAMA Network Open. 2020; 3(11): e2024352. Retrieved from https://jamanetwork.com/journals/jamanetworkopen/fullarticle/2773396
- Waldman, S.D. (2014). Cubital Tunnel Syndrome. Atlas of Uncommon Pain Syndromes (Third edition). Retrieved from https://www.sciencedirect.com/topics/medicine-and-dentistry/cubital-tunnel-syndrome
- Radial Tunnel Syndrome. (2015 January 29). Cleveland Clinic. Retrieved from https://my.clevelandclinic.org/health/diseases/15658-radial-tunnel-syndrome









