
Frenums are normal anatomy within the mouth, yet often neglected. The frenum consists of loose, fibrous connective tissue, elastic fibers, and striated muscle fibers that develop from muscle bundles of the lip. The purpose is to provide stability to the tongue and upper and lower lip.
This mucous membrane fold attaches the lip and cheek to the alveolar mucosa, gingiva, and underlying periosteum. The mouth consists of a buccal, labial, and lingual frenum.1,2
Buccal Frenum
Buccal frenums are thin strands of tissue connecting the gums to the inside of the cheeks, commonly located at the premolar area. This frenum may pull tightly in the cheeks, giving it the potential to contribute to oral motor dysfunction — the challenge of controlling mouth muscles for proper function. The constant tug of the frenum may pull on the tissue around the teeth and causing deep pockets.1
Labial Frenum
Labial frenums are connective webbing that attaches the upper (see Figure 1) or lower lip to the gingiva at the top of the front teeth in the maxillary and below the front teeth in the mandible. It should be attached at least 4 mm above the crest of the front teeth and should not limit lip movement. About 10% of children will have the labial frenum into the papilla.3
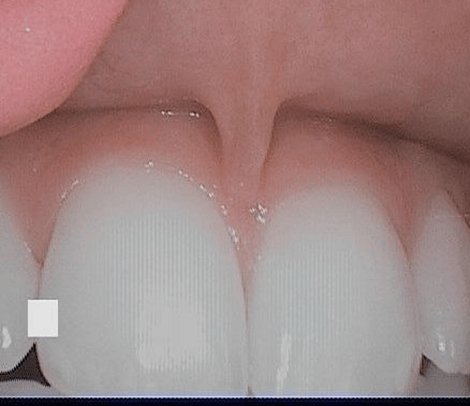
To check for abnormal frenum attachment, the blanch test can be performed along with an examination of the clinical appearance of attachment. The blanch test is performed by lifting the lip and pulling it outwards. The appearance of blanching indicates a high labial frenum attachment.
Complications of a Maxillary Tight or Low Labial Frenum
Diastema − A diastema is a space or gap wider than .5 mm between the teeth. It may be considered a cosmetic flaw or a source of character. It can be between any teeth, yet the frenum related version is commonly between maxillary or mandibular incisors. A tight or low labial frenum is what causes the majority of the anterior diastemas.
Nursing − It can cause complications in latching, therefore making nourishment a concern.
Recession − As the lip moves, the frenum is continually tugging on the papilla, which can eventually pull the tissue down on the teeth.
Open mouth posture − The tight ligament limits lip function, preventing it from adapting with the lower lip to forming a lip seal when closing the mouth. This can cause a person to mouth breath. In children, it can contribute to abnormal jaw growth and airway development.
Poor oral home care − With a tighter and low frenum, it may cause limited or a tight lip against the teeth, resulting in a higher risk for biofilm, decay, and gingivitis in the anterior teeth.3

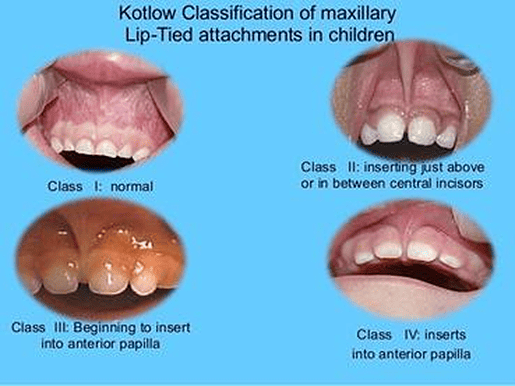
Dr. Kotlow’s Classifications of Labial Frenum (see Figure 2)
- Mucosal (Class 1): the frenal fibers are attached up to the mucogingival junction
- Gingival (Class 2): the fibers insert within the attached gingiva
- Papillary (Class 3): the fibers extend into the interdental papilla
- Papilla penetrating (Class 4): the fibers cross the alveolar process and extend up to the palatine papilla2,4
Lingual Frenum
A lingual frenum is a vertical band of thin tissue located under the center of the tongue that connects the tongue to the base of the mouth.2 Its function is to anchor and stabilize the tongue.
Complications of a Tight Lingual Frenum
Low tongue position − Low tongue position causes the tongue to lie lower in the mouth, causing the abnormal growth of the lower jaw and insufficient upper jaw growth. This may result in severe future orthodontics issues and sleep apnea.
Swallowing and dysfunction − When swallowing, the tongue should rest against the upper palate vault. If a tight frenum is present, it is unable to reach that high, and the tongue will tend to want to rest between the teeth to cause tongue thrust. A tongue thrust is an oral myofunctional disorder where the tongue protrudes anteriorly or laterally during speech, swallowing, or at rest. This can cause an open anterior bite.

Speech challenges and lisping − Lisping is caused by wrongful tongue placing. This causes a speech impediment with mispronouncing certain letters such as “s, z, t, d, l, j r, I, ch, th, zh, and dg.”
Interferes with denture stability − When the tongue moves, the frenum attachment may tense up, causing the lower denture to move.
Tongue-tie – Tongue-tie is also referred to as ankyloglossia and is a short, lingual frenum where the tongue is more closely attached to the bottom of the mouth. It is usually an abnormally short, thick frenum attached to the tip of the tongue. The tip of the tongue will be notched or heart-shaped when it is protruded.
This condition leads to trouble during breastfeeding, difficulties eating (licking foods such as ice cream), sticking the tongue out past the lower front teeth, lifting the tongue to the upper teeth, or moving it side to side. It may also cause challenges while playing certain instruments. Tongue-tie is more common in males than in females.4,7

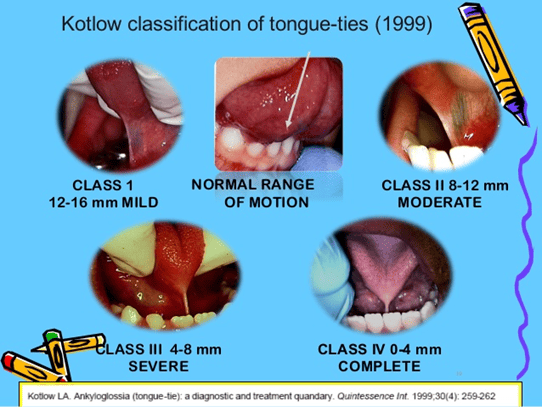
Dr. Kotlow’s Tongue-tie Classifications (see Figure 3)
Dr. Kotlow’s assessment is based on the length of the tongue from the insertion of the lingual frenum at the base of the tongue to the tip of the tongue.
- Class 1: Mild ankyloglossia (12-16mm)
- Class 2: Moderate ankyloglossia (8-12mm)
- Class 3: Severe ankyloglossia (4-8 mm)
- Class 4: Complete ankyloglossia (less than 3mm)
Frenum Surgeries
Frenectomies are the complete removal of a frenulum, including its attachment to the underlying bone. Usually performed at the labial frenum or the lingual frenum, it is a common dental procedure on infants, children, and adults.
The surgeries are usually recommended when they interrupt a person’s way of life. The indications for frenum removal is an abnormal attachment causing a midline diastema, a flattened papilla with a closely attached frenum to the gingival margin, causing recession, and an abnormal frenum with an inadequately attached gingiva and a shallow vestibule.4
Frenectomies are usually short surgeries with a quick recovery. These procedures, depending on its purpose, will be performed by scalpel, electrosurgery, or lasers.
A lingual frenectomy is usually related to ankyloglossia. A labial frenectomy is common with diastemas and denture procedures to provide a proper fit. In infants, a frenectomy is performed if there are tongue-tie or lip ties that interfere with feeding.
Frenum Procedure Techniques
Conventional or classical: Common procedure with midline diastema involvement.
Miller’s: Proposed for the post-orthodontic diastema. This surgery is done after the orthodontic movement is complete and about six weeks before the appliances are removed. This a win-win for allowing healing and tissue maturation, but also the orthodontics appliances retain the periodontal dressing. This technique results in maintaining the interdental papilla without scarring.4
V-Y plasty: Indicated for lengthening the localized area when a broad frenum is in the premolar-molar area.4
Z plasty: Indicated for a thick hypertrophic frenum associated with an inter-incisor diastema and a short vestibule. This achieves both removal of the fibrous band and vertical lengthening of the vestibule.4
Electrosurgery: Is recommended when bleeding disorders are present, and the traditional scalpel carries a higher risk with problems achieving bleeding control.4
Frenuloplasty: Is the surgical alteration of a frenum when it restricts the range of motion. The common area is the tongue.4
Frenotomy: Is the incision and relocation of the frenal attachment to create an area of attached gingiva between the gingival margin and the frenum.2,4
Frenum Piercings
Oral piercings are high risks of causing gingival recession, teeth erosion, enamel damage, infection, and allergies. With a foreign object constantly rubbing on the gums and teeth through natural or unnatural mouth movements, it causes damage to the target areas. Infection may be higher at the piercing site, so home care is important to keep that minimized. Jewelry migration is particularly high for lip frenum piercings due to the thinness of the frenum and a small area.
A lip frenum piercing is either at the upper or lower lip. The upper lip piercing is called a smiley or scrumper since it is noticed when the person smiles. The lower lip is oppositely known as a frowny. The lingual frenum is pierced horizontally with a bar or ring.7
Frenum Variations
- Simple with a nodule
- Simple with an appendix
- Simple with nichum
- Bifid labial frenum
- Persistent tectolabial frenum
- Double frenum
- Wider frenum usually covers two teeth2,6
Frenum Injuries
Frenum tears, rips, or traumas are not uncommon. A torn or ripped frenum may happen from injury or trauma to the mouth or face. A torn frenum can be caused by an object forcefully entering the mouth, aggression with the toothbrush, being pulled, snagged, eating, kissing, oral sex, or orthodontic treatment. It may be common in young kids as they fall and hit their faces often. It’s also something to be aware of since evidence of physical trauma may be a sign of physical abuse. In physical abuse, a torn frenum has been reported in 49% of infants and 38% in toddlers. The lingual frenum heals well on its own, but around the frenum, its highly vascular, which may induce a bleeding problem.7
More often than not, the frenum may be overlooked. While frenums are not a source of diagnosing disease, illnesses, or systemic risks, it’s just as important to determine for dental concerns. Frenums that can cause problems are usually diagnosed and treated in children, so by adulthood, dental-related frenum concerns are very minimal.
Now Listen to the Today’s RDH Dental Hygiene Podcast Below:
Frenum References
- Morgan, B. Tongue, Lips and Cheek Ties. MOB, Motherhood International. 2019. Retrieved from http://www.mobimotherhood.org/tongue-and-lip-ties.html.
- Priyanka, M., Sruthi, R., Ramakrishnan, T., Emmadi, P., Ambalavanan, N. An overview of frenal attachments. Journal of Indian Society of Periodontology. 2013; 17(1): 12-5. 10.4103/0972-124X.107467.
- Abnormal Frenum Attachments in Children. Homeopathic Dentistry. April 24, 2016. Retrieved from https://www.homeopathic-dentistry.com/475/abnormal-frenum-attachments-in-children/.
- Devishree, Gujjari, S.K., Shubhashini, P.V. Frenectomy: a review with the reports of surgical techniques. J Clin Diagn Res. 2012; 6(9): 1587-1592. doi:10.7860/JCDR/2012/4089.2572. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3527809/.
- Tongue-tie (ankyloglossia). Mayo Clinic. Retrieved from https://www.mayoclinic.org/diseases-conditions/tongue-tie/symptoms-causes/syc-20378452.
- Jindal, V., Kaur, R., Goel, A., Mahajan, A., Mahajan, N., Mahajan, A. Variations in the frenal morphology in the diverse population: A clinical study. J Indian Soc Periodontol. 2016; 20(3): 320-323. doi:10.4103/0972-124X.182598.
- Seladi-Schulman, J. How to Treat and Prevent Conditions of the Lingual Frenulum. September 4, 2019. Healthline. Retrieved from https://www.healthline.com/health/lingual-frenulum#tear.









