
From the geometry of instrumentation angulations, biofilm index calculations, as well as the mean, median, and modes of research, we can’t escape math even in the dental hygiene world. As you know, some of the more challenging math equations are in dental anesthesia. The milligrams versus milliliters and moving the decimal points can be quite the challenge.
The three main calculations of dental anesthesia are reviewed in this article.

While temping at an office where I was to provide all of the anesthesia for the dentist’s procedures, the schedule that day was third molar extractions. One patient was a 100-pound, 16-year-old female. The assistant passed me a tray full of carpules and said, “Here are your 21 carps.”
“21 carps?” I questioned.
“Yes, that’s what the usual hygienist gives,” the assistant stated, seemingly a little concerned about my skills. As I was in a time crunch, I proceeded to get all areas anesthetized with one carpule for each nerve block. As the local anesthesia took effect, I quickly did the math to see how much I could give her based on her weight.
I have memorized the Food and Drug Administration’s (FDA) maximum recommendation of mg/lb for lidocaine (see Table 1) and multiplied it by the patient’s weight in pounds (lbs), giving me the total maximum recommended dosage (MRD) for her weight.
Maximum Recommended Dosage Calculation2
Maximum recommended dose (from FDA) mg/lb x patient’s weight (lbs) = MRD
| Anesthetic Drug | mg/lb | mg/apt |
| Articaine | 3.2 | NA |
| Bupivacaine | 0.9 | 90 mg |
| Lidocaine | 3.2 | 500 mg |
| Mepivacaine w/wo | 3.0 | 400 mg |
| Prilocaine w/wo | 3.6 | 600 mg |
Table 1 MRD from FDA. Adapted from Malamed1
For my patient, 3.2mg/lb of lidocaine x 100 lbs = 320 mg was her maximum recommended dose versus the 500 mg that should not be exceeded regardless of body weight.
Watch how to get the maximum recommended dose in our video on Hygiene Edge.
SPECIAL NOTE: If another type of anesthetic is added, you would go with the lowest MRD between the differing anesthetics. This calculation is explained in a Hygiene Edge video.
Milligrams per Cartridge Calculation2
So now, how do I translate 320 mg into the number of carpules I am supposed to use? The first step to get this calculation is to note the drug concentration percentage written on the carpule; it will be either 0.5%, 2%, 3%, or 4%. Then do the following calculation to determine how many milligrams are in just one cartridge.
Concentration% (0.5%, 2%, 3% or 4%) x # of carps x 18 (cartridge volume) = mg/cartridge
So for my patient, 2% lidocaine x 1 carpule x 18 = 36 mg per cartridge.

The second step is to determine how many carpules you can use. For my patient, I divided 320 mg (MRD) by the 36 mg in one carpule of lidocaine and found that she could have 8.8 carpules vs. the 21 given to me.
See how important it is to get that right? I might have given her an overdose if I hadn’t done the math.
A Hygiene Edge video further explains this calculation.
Document the Math
I am all about efficiency, so I have made myself a quick reference guide for office anesthesia. I’d recommend you do the same for your practice as well as anesthesia protocols on documentation and taking and recording blood pressure.
As a new dental assistant back in 2002, I was taught to document injections administered simply as Anesthetic: 1 carp lido. I now realize the importance of proper documentation in case of a medical emergency or for reference in case of other complications.
Have an office meeting and decide what’s best for your practice but consider adding in the following:
- The injection(s) given
- Needle(s) used, including gauge and length
- Local anesthetic drug used
- Dose (in milligrams) of the solution(s) used
- Vasoconstrictor used (if any)
- Patient’s reaction1,2
A chart note example of this may be: R-IANB, 25-long, 2% lidocaine (36 mg) with 1:100,000 epinephrine, tolerated procedure well.
Vasoconstrictor Dose Calculation
Wait a second! Did you notice that documentation of the vasoconstrictor is needed? Guess what? That has some math too. Let’s review what to do if you have a patient with a condition that requires you to limit epinephrine. In this case, you must use the vasoconstrictor dose, sometimes called cardiac dose or epi dose.
When I was an assistant, I once had a patient’s chart that said in big red letters: NO EPI. That patient needed an extraction, but the “plain” anesthetic was not cutting it. The dentist asked me to hand him a carpule of lidocaine.
I pointed to the big red letters, and that’s when the dentist educated me about the vasoconstrictor dose. He said, “If we follow certain guidelines, the patient will be just fine. The constant pain the patient is currently experiencing is naturally putting an extra load on the cardiovascular system. So we will only give the vasoconstrictor dose.”
I was grateful that the patient was able to get out of pain for the procedure and receive the care they needed.
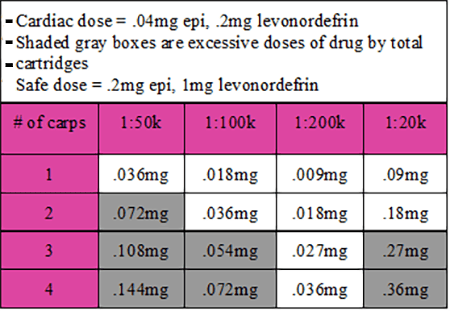
The vasoconstrictor (VC) dose is based on dilution ratios versus percent of concentration and is not dependent on the patient’s weight. For epinephrine, the standard safe dose is 0.2mg and 1 mg levonordefrin. Yet the cardiac dose is much lower at .04 mg for epinephrine, and for levonordefrin, it is 0.2 mg.1,2
To calculate milligrams of vasoconstrictor, you first look at the dilution ratio of the vasoconstrictor. The carpule will say one of the following: 1:50,000, 1:100,000, 1:200,000 epinephrine, or 1:20,000 levonordefrin.
Second, convert these ratios to milligrams per milliliter. Table 2 below shows conversions for each ratio.
| 1:20,000= .05 mg/ml | levonordefrin | five times as much VC as a 1:100k solution |
| 1:50,000= .02 mg/ml | epinephrine | twice as much VC as 1:100k solution |
| 1:100,000= .01 mg/ml | epinephrine | compare other solutions to this 1:100k |
| 1:200,000= .005 mg/ml | epinephrine | half as much VC as 1:100k solution |
Table 2 Vasoconstictor conversions for each ratio. Adapted from Malamed1
You will then do the following calculation2:
mg/mL converted ratio x 1.8 mL solution x #of carps = vasoconstrictor dose mg
Let’s plug some real numbers in: .01mg/ml x 1.8ml x 1 = .018.
This number is well below the .04mg of epinephrine that a cardiac patient can have. In another example, let’s say you wanted to give three carpules that have 1:50,000 epinephrine. This calculation would be: .02mg/ml x 1.8 ml x 3 = .108
This calculation is also elaborated on in this Hygiene Edge video. I am within the standard safe dose of .2 mg but above the .04.
Personally, I like to use the quick reference below (Table 3) so that I don’t have to do this math as often.
It is very rewarding to be able to give local anesthesia to patients to get them comfortable for procedures. The math does take practice, practice, practice. But I promise that it becomes easier the more you do it.
Before you leave, check out the Today’s RDH self-study CE courses. All courses are peer-reviewed and non-sponsored to focus solely on high-quality education. Click here now.
Listen to the Today’s RDH Dental Hygiene Podcast Below:
References
- Malamed, S.F. (2020). Handbook of Local Anesthesia (7th ed.). Elsevier.
- 2. Bassett, K.B., DiMarco, A.C., Naughton, D K. (2015). Local Anesthesia for Dental Professionals (2nd ed.). Pearson Education, Inc.










