
Early childhood caries (ECC) is one of the most common chronic childhood diseases, and possibly the most preventable. The American Academy of Pediatric Dentistry (AAPD) defines ECC as a significant chronic disease resulting from an imbalance of multiple risk and protective factors over time1. In the United States, 3-6% of children under the age of 6 are affected by ECC which can lead to pain, low self-perception, and speaking and eating issues. Early childhood caries also puts the permanent adult dentition at five times greater risk of developing decay4. Dental hygienists have an important role in educating parents and children about this disease and have an opportunity to help decrease the prevalence of ECC with preventive therapies.
Early childhood caries is classified as one or more decayed, missing, or filled tooth surfaces in any primary tooth in a child under six years old. Smooth surface caries present in a child younger than three years old is considered severe ECC3. The enamel of primary teeth is half the thickness of permanent teeth, with a less organized microstructure, that may be more easily demineralized by plaque acids4. Streptococcus mutans is the most common microorganism associated with early childhood caries. In addition to several other bacteria, fungi, such as Candida albicans, are now also recognized as taking part in the progression of dental caries.

Microorganisms developed in poly-species biofilms produce exopolysaccharides or extracellular polymeric substances that allow bacteria to resist antimicrobials. These bacteria may exist without detriment, but combined with risk factors such as a diet high in sugars and fermentable carbohydrates, saccharides are absorbed and metabolized to produce lactic acid1.4. The shift in oral pH from neutral to acidic creates a microbial imbalance and perfect environment for dental caries progression.
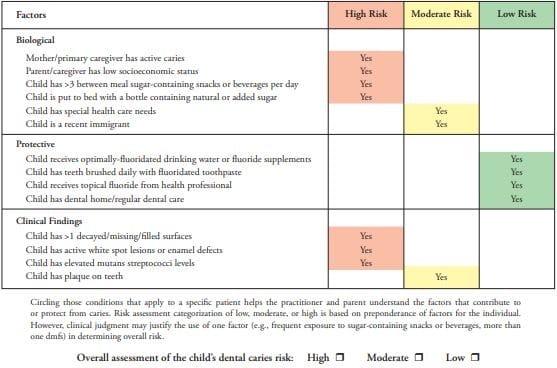
There are several risk factors for the development of early childhood caries including microbiological, environmental, and dietary. The most common contributing factors are improper feeding practices, familial socioeconomic background, parental lack of education in oral health, and lack of access to care2. Vertical transmission of bacteria from parent or caregiver or horizontal transmission from other family or children in school may encourage earlier development of ECC. Depending on the frequency and amount of exposure, children whose mothers have saliva containing Streptococcus mutans are at a much higher risk of developing caries early in life1. The AAPD’s Caries Risk-Assessment and Management for Infants, Children and Adolescents provides a chart to assess a child’s risk of developing early childhood caries.
Table 1. Caries Risk Assessment for Children Aged 0-5 for Dental Providers
Dental hygienists have a vital role in early childhood caries prevention through education. Education can begin early with expectant parents. The American Academy of Pediatric Dentistry’s Policy on Early Childhood Caries: Classifications, Consequences and Preventive Strategies recommend these topics for educating new parents on prevention:
- Avoiding frequent consumption of liquids or foods containing sugar including milk/formula especially at bedtime.
- Begin oral hygiene no later than the eruption of the first primary tooth, begin massage of the gums prior to eruption to get the baby used to oral hygiene care.
- Establish a dental home within six months of the eruption of the first tooth and no later than one year of age (even if only to assess caries risk and provide education).
- Work with other medical providers to ensure children access to screenings and care.
There are suggested goals of the initial dental hygiene visit with young children outlined by the AADP’s Policy on the Role of Dental Prophylaxis in Pediatric Dentistry:
- Instruct caregiver and child in proper oral hygiene techniques.
- Remove plaque, extrinsic stain and calculus deposits.
- Examine hard and soft tissues.
- Introduce dental procedures to the young child.
Long-term preventative goals for dental hygienists are to reduce dental plaque formation, change the composition of existing plaque bacteria, and hopefully modify detrimental dietary habits through parental education2.
Management of children who suffer from ECC is also very much about prevention. After necessary restorations, dietary counseling with caregivers, and promoting good oral hygiene and feeding habits at home, are essential to preventing new caries. Children with existing caries have 5-6 times greater prevalence of new caries than caries-free children4. Interventions such as fluoride, casein phosphor peptide (CPP) and amorphous calcium phosphate (ACP) can prevent tooth demineralization and improve enamel remineralization2. Xylitol products are also a perfect substitution for more common sweeteners. The sugar alcohol is absorbed and metabolized like a saccharide, but no acids are produced from the spent energy.
Early childhood caries is highly preventable if caregivers, parents, and other healthcare professionals are educated about the importance of the primary dentition, and if good habits are introduced early. Dental hygienists are in a pivotal position with the ability to reduce the prevalence of ECC by providing oral health education, preventive care, and forming relationships with the healthcare community to increase access to care.
SEE ALSO: Science Confirms Water Fluoridation Prevents Tooth Decay in Children
DON’T MISS: Ask Kara RDH: Only Polishing Children & Considering it a Child Prophy
References
- 2018-19 Definitions, Oral Health Policies, and Recommendations. (n.d.). Retrieved from http://www.aapd.org/policies/
- Anil S, Anand PS. Early Childhood Caries: Prevalence, Risk Factors, and Prevention. Frontiers in Pediatrics. 2017;5:157. doi:10.3389/fped.2017.00157.
- Kayalvizhi, G., Nivedha, D., Sajeev, R., Prathima, G. S., Suganya, M., & Ramesh, V. (2017, February 1). Evaluating the Efficacy of Xylitol Wipes on Cariogenic Bacteria in 19- to 35-month-old Children: A Double-blind Randomized Controlled Trial. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5968156/
- Meyer, F., & Enax, J. (2018, May 22). Early Childhood Caries: Epidemeology, Aetiology, and Prevention. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5987323/#B90









 Dental Hygiene School")